Episode Transcript
Interviewer: What is abdominal aortic aneurysm, how did you end up with it, and what can be done about it? We'll talk about that next on The Scope.
Dr. Claire Griffin is a vascular surgeon with the University of Utah Health and one of the things that you deal with on occasion or often—I guess we'll find out—is an abdominal aortic aneurysm, also called "AAA." So what is that?
Dr. Griffin: Well, an aneurysm is when a blood vessel becomes larger than it should be. So we define in medicine an aneurysm as any time the blood vessel is one and a half times the normal size.
Now, normal is different depending on the patient, how big they are, if they're a man or a woman. But in general, we have an idea of how big blood vessels should be, and when they're larger than that, we call them aneurysmal.
Interviewer: All right. You get a little bit concerned about it. Let's go back for one more step. What exactly is the aorta? Where is this happening in my body?
What Is an Aortic Aneurysm?
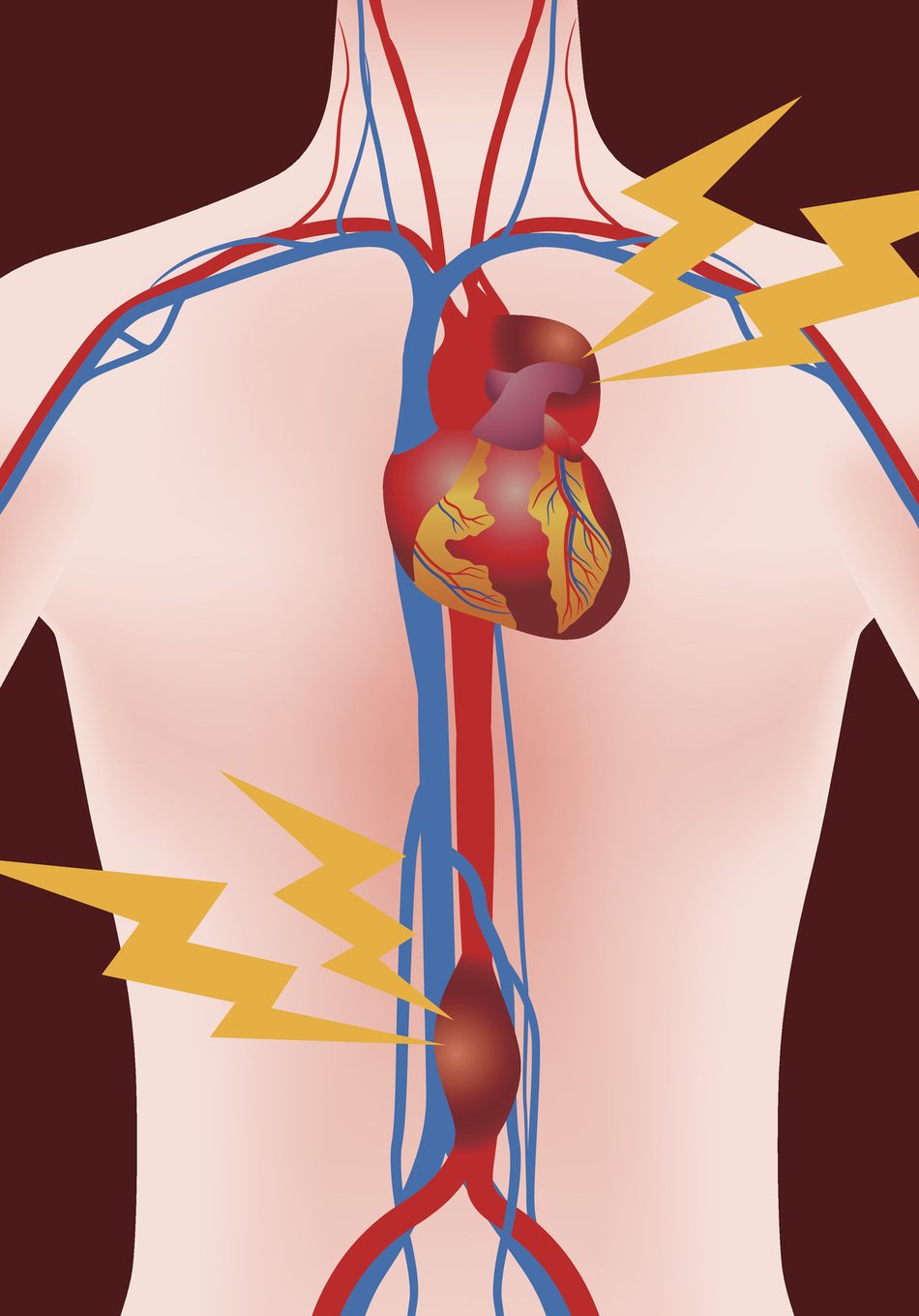
Dr. Griffin: Okay. So you can get an aneurysm in any blood vessel in the body but the most common location is in the abdominal aorta. So the aorta is the main blood vessel in our body. It actually starts in the chest where it comes directly off of the heart and it gives branches to the arms and the head before traveling through the chest and going into the abdomen.
There are actually two main branches that come off of the aorta right after it gets into the abdomen that give blood to the liver and the intestines and then another branch goes to each kidney. Once those branches have come off there's a relatively straight section of the aorta before it divides into two around the level of our belly buttons to give blood flow to our pelvis and our legs. So that's the aorta in a nutshell, the main blood vessel or the superhighway for blood to get from the heart to everywhere else in our body.
AAA or Abdominal Aortic Aneurysm
Interviewer: So then piecing together what you've just told us, an abdominal aortic aneurysm is when the aorta in the abdominal area is larger than it should be?
Dr. Griffin: Exactly.
Interviewer: All right. So can you explain that a little bit further?
What Is the Normal Size of the Abdominal Aorta?
Dr. Griffin: Sure. So the normal size of the aorta depending, again, on if you're male or female or how big you are is normally about 1.7 centimeters to 2.5 centimeters. Which given that we don't use centimeters very often, really means about the size of a nickel.
When we see somebody who has an aorta that is bigger than three centimeters, so around the size of a half dollar, we consider that to be an aneurysm. Now, having an aneurysm doesn't mean that you need anything done about it. It really depends on where it's located and how big it is.
Interviewer: All right. And what caused this aneurysm to happen? Was it something that I did or does it just happen?
What Causes Abdominal Aortic Aneurysm?
Dr. Griffin: So we know that there's definitely some sort of genetic component aneurysm disease but there's not one gene that causes them to happen. It's really multi-factorial.
We know for example that smoking is like fertilizer for aneurysms and causes them to grow really fast. So the number one thing we can do is avoid smoking to prevent them from happening. But even if you've never smoked, you can still have aneurysm. And if your parents or grandparents had one or uncles or aunts had one, that is a risk factor for you.
Interviewer: So how is it diagnosed?
AAA Screenings
Dr. Griffin: Because we know that smoking is the most common risk factor, there actually are screening programs that if you are a male over the age of 65 and you've been a smoker in your life, you can get an ultrasound to look at the size of your aorta. Although the most common way this is diagnosed is because people get a CT scan for something completely unrelated and it's found by accident on a CT scan.
Interviewer: So it doesn't really present any noticeable symptoms that . . . like shortness of breath or something like that. It just . . .
Dr. Griffin: No. If they're quite large, they can present symptoms because of their size or if they grow rapidly, sometimes patients will have pain associated with that, but they are most commonly asymptomatic.
Interviewer: All right. And kind of found by mistake.
Dr. Griffin: Exactly.
Interviewer: Because you're looking for something else. So when does it become a problem?
Dr. Griffin: So as the blood vessel, in this case the aorta, stretches it doesn't get any thicker. So the wall just becomes thinner and thinner. Sometimes that growing can cause abdominal pain but usually it's asymptomatic. Once it gets to a certain size, we worry that that thin wall can actually become so weak that the blood leaks out of it and that can be an emergency, considered a rupture. So we like to fix them before it gets to the size where it would rupture.
Interviewer: Yeah. And if it ruptures, then like you said, that's an emergency. That's your blood gushing out now at this point.
Dr. Griffin: Correct.
Interviewer: Pretty quickly, I'd imagine.
Dr. Griffin: It can be what we would call a contained rupture where you have some sort of symptom and pain, but even if it's a contained rupture it's still a surgical emergency to fix it.
Interviewer: So if a patient is diagnosed with one, what then? You mentioned not in all cases do you have to do something but . . .
Treatment for AAA
Dr. Griffin: Depending on the size of it dictates what the next step is. So if we diagnose it and it looks like it has already met the threshold for repair, in other words, if we think that continuing to live with it is more risky than fixing it, we go ahead and do surgery to fix it. But if your aneurysm is small, it might be that you never need it fixed and so we continue to watch that or place it in surveillance and do serial imaging with either ultrasound or CT scan to keep an eye on it.
Interviewer: And then how and when do they get fixed? You'd mentioned you kind of keep an eye on it, right? If it gets stretched so far, that's when it gets fixed. So then what do you do, is it surgery?
Dr. Griffin: There are no medicines that fix aneurysms. The only thing that we can do is reroute the blood somehow so that the high blood pressure isn't touching this thinned out wall. There are two different ways that we can fix it:
- We can either open up the patient in the operating room and replace that thinned out blood vessel or the enlarged area of the aorta or
- If the anatomy is right, which is something that we can tell on a CT scan, we can actually travel inside the blood vessels through specialized IVs and re-line the blood vessel so that the thinned out wall is no longer getting the pressurized blood.
And depending on how we fix it, it has a lot to do with how fast the recovery is and when you can get back to your normal life.
Interviewer: After you've been diagnosed, is it . . . are you pretty good for the most part in your specialty at being able to know, "We need to do some about this right now or we have a couple of weeks?"
Dr. Griffin: Yeah. So the Society of Vascular Surgery actually has some really great guidelines that help us make decisions about patients and every patient is different. So I mentioned before how there are branches that come off the aorta. If the aneurysm includes those branches, that can make it a very complicated surgery to fix it. Or if the aneurysm is away from those branches, it can be a very straightforward repair.
So the CT scan that we usually get to diagnose it and to surveille it is critical in helping us decide how to treat it.
Interviewer: Okay. I guess what I was trying to figure out is if I was told I have an aneurysm, to me, that's an emergency, like right now. But you have a pretty good body of evidence that kind of helps dictate how dangerous you are at any given time.
Find a Vascular Specialist to Help You
Dr. Griffin: Exactly. And since this is something that I treat all the time, as a vascular surgeon, when I hear that somebody has an aneurysm, that is part of what I take care of every day. So I don't think that patients should be scared or think that it's an emergency to fix it right away. On the other hand, it is important to get plugged into a vascular surgeon so that they can tell you when and how and what the next step was going to be.
updated: August 13, 2021
originally published: August 22, 2017