What Is a Skull Base Tumor?
Traveling to Utah?
Let us help you navigate your visit.
COVID-19 Information
Find information about COVID-19 safety at U of U Health.
Skull base tumors all have one thing in common: They are a mass located next to or involving the skull bones. This mass often grows near the bottom of the brain or behind the eyes, nose, and ears.
A variety of skull base tumors exist. They typically grow inside the skull or nose/sinuses, although some grow on the exterior. They can be benign (noncancerous) or malignant (cancerous) depending on the type.
Symptoms of skull base tumors vary and can develop slowly over time.
Is a Skull Base Tumor a Brain Tumor?
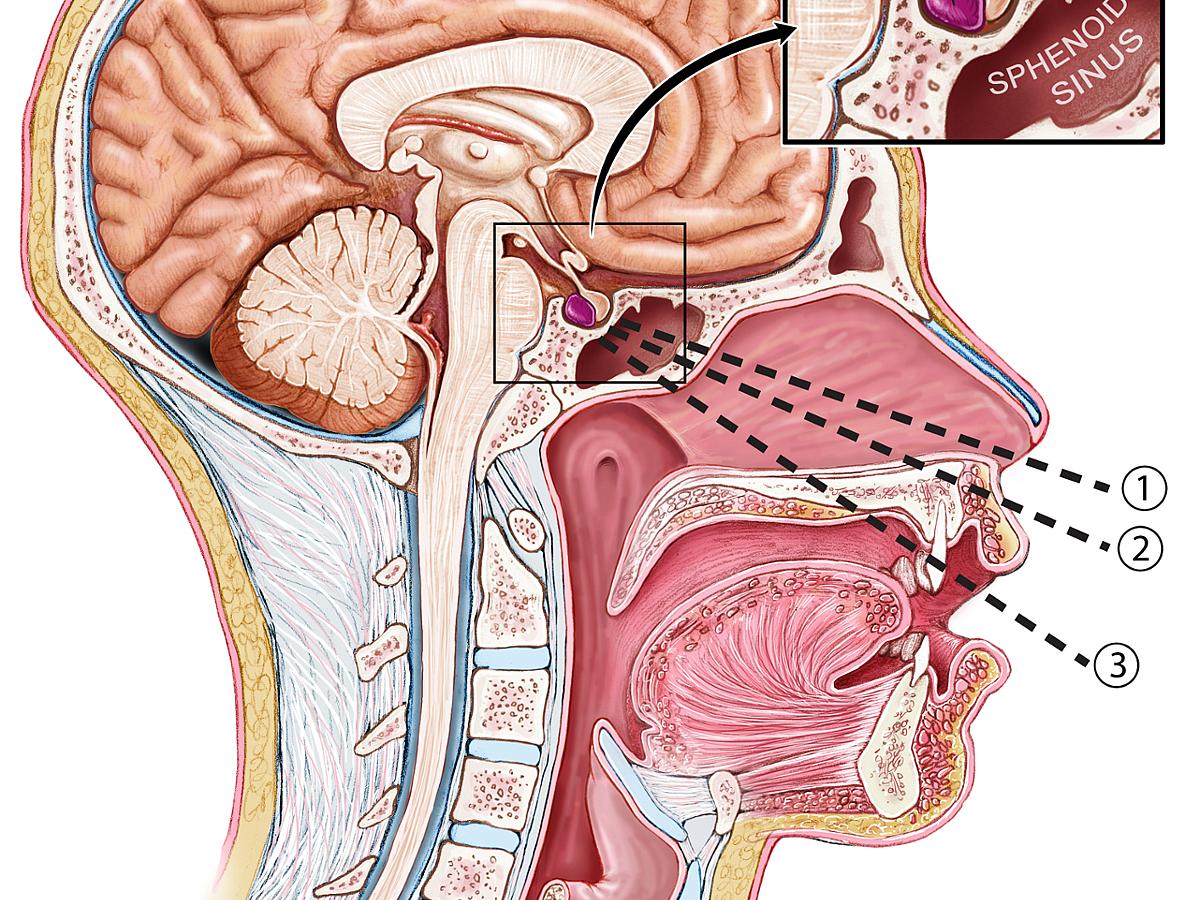
Generally no, but it may be growing in a variety of places — not just inside the brain. These tumors do not start in brain tissue but grow next to the brain and may put pressure on neural structures. A tumor may be at the base of the brain or on the back of the skull. It may be growing in the front — near the eye sockets in the nose and sinuses — or in the pituitary gland, among other locations.
Are All Skull Base Tumors Cancerous?
No. Just because a tumor has grown inside your body does not necessarily mean you have cancer. Many tumors are benign (non-cancerous).
Skull Tumor Symptoms
Each patient may feel differently depending on the location of the tumor, its size, and type.
Location
Location is extremely important. A large tumor in some areas of the skull will have less impact than a small tumor in the base near the nerves and carotid artery.
Size
Tumors can range in size from less than one centimeter to many centimeters in diameter. Symptoms may appear once the tumor has grown to a certain point and places pressure on the brain and nerves, affecting normal body functions.
Type
There are two common types of skull base tumors: lateral and anterior.
Can You Feel a Skull Base Tumor?
Typically not. Lumps on the head may be a sign of something else such as a head injury or other conditions. Those include a noncancerous cyst, an inflamed hair follicle, or a noncancerous skin tumor.
Lateral Skull Base Tumors
Lateral skull base tumors are at the back of the skull base and are typically benign. Some examples include:
- Acoustic Neuromas—Noncancerous tumors growing on the nerve leading from the inner ear to the brain. Slow growing.
- Meningiomas—A tumor found on the tissue covering the brain or spinal cord in the skull interior. Typically benign. These can also be anterior tumors.
- Paragangliomas—Found in the head and neck. Rarely cancerous.
Symptoms of Lateral Skull Base Tumors
Common symptoms of lateral skull base tumors include:
- hearing loss,
- headaches,
- balance problems,
- problems swallowing, and
- voice hoarseness.

Anterior Skull Base Tumors
Anterior skull base tumors are found in the front of the skull base near where the eye sockets and sinuses are located. Some examples include:
- Meningiomas—A tumor found on the tissue covering the brain or spinal cord in the skull interior.
- Pituitary tumors—Tumors in the pituitary gland, which is located in the area behind the nose. They are also typically benign but can cause an increase or decrease in hormone levels.
- Esthesioneuroblastomas—Tumors found in the upper nasal and sinus cavities.
- Sinonasal squamous cell carcinomas
- Sinonasal adenocarcinomas
- Sinonasal mucosal melanomas
- Sinonasal adenoid cystic carcinomas
- Sinonasal undifferentiated carcinomas
- Sinonasal neuroendocrine tumors
- Juvenile nasopharyngeal angiofibromas
- Inverted papillomas

Symptoms of Anterior Skull Base Tumors
Common symptoms include:
- vision and eye movement problems,
- weight loss,
- muscle weakness,
- reduced menstrual periods (pituitary tumors),
- erectile dysfunction (pituitary tumors),
- reduced sense of smell,
- nosebleeds,
- congestion (sometimes on one side),
- sinus infections, and/or
- problems breathing through your nose.
Consultations
Lateral Tumors
- Acoustic Neuromas
- Meningiomas
- Paragangliomas
Anterior Tumors
- Meningiomas
- Pituitary tumors
- Esthesioneuroblastomas
- Sinonasal squamous cell carcinomas
- Sinonasal adenocarcinomas
- Sinonasal mucosal melanomas
- Sinonasal adenoid cystic carcinomas
- Sinonasal undifferentiated carcinomas
- Sinonasal neuroendocrine tumors
- Juvenile nasopharyngeal angiofibromas
- Inverted papillomas
Find a Specialist
Causes & Diagnosis
Causes
No one knows the exact causes of skull base tumors, but certain genetic conditions or exposure to some chemicals may increase risk. Radiation therapy to the head, brain, or neck can also be a risk factor.
Diagnosis
Determining whether or not a patient has a skull base tumor takes several steps. These include an overall physical exam, neurological tests, and imaging tests to look inside the skull and in or around the brain.
Physical Exam
To decide whether a patient has a skull base tumor, doctors will begin with a physical exam to better understand a patient’s symptoms and history.

Neurological Exam
Doctors will also perofrm neurological exams to learn more about any changes to other parts of your body.
If we suspect an anterior skull base tumor, we will test for:
- vision,
- reflexes,
- coordination, and
- memory and cognition.
For lateral skull base tumors, we will test your:
- hearing,
- balance, and
- coordination.
Imaging
Specialized tests help doctors understand where and if a skull base tumor exists. To see inside the skull and brain, physicians may order magnetic resonance imaging (MRI), a bone scan, positron emission tomography (PET), or computed tomography (CT or CAT scan).
A neuroradiologist, who specializes in problems of the head, neck, brain and spine, will review the images that a skull base surgeon may need. Because many tumors have strong visual characteristics, imaging often allows doctors to confirm a tumor type before any surgery has taken place.
Biopsy
In some cases, our doctors will perform a biopsy — the removal of a small piece of tissue — to help confirm a skull base tumor diagnosis. This may happen before surgery. Once tumors are removed, they are always sent to the lab for further analysis.
Treatment for Skull Base Tumors
At University of Utah Health, treatment for skull base tumors depends on your unique circumstances. The tumor size, location, and your overall age and health will help you and your specialist determine the best treatment.
Your treatment choices may include:
- waiting and observation (noncancerous tumors only),
- surgery,
- radiation, and
- in some cases chemotherapy.
Observation
For some patients with benign (noncancerous) tumors, we may recommend waiting to see if and how the tumor changes. We will monitor and measure the tumor’s growth over time. If the size remains the same and your symptoms are not significant, we may recommend no additional treatment.
Some tumors stop growing in older patients or grow so slowly that they will not be a problem in the patient's lifetime.
Surgery
Surgery depends on the location of the tumor, its size, and how it affects you.
Anterior Skull Base Surgery
The location of the tumor, its size, and how it affects you, will help us determine if surgery is the best treatment choice. If so, there are two main approaches for anterior based tumors:
- endoscopic endonasal surgery.
- traditional brain surgery, known as an open craniotomy.
A team of doctors works together to remove the tumor and achieve the best outcome for you. Members of that team can include:
- a neurosurgeon,
- a rhinologist, and
- an anesthesiologist.
Endoscopic Surgery
Skull base surgeons can remove many skull base tumors with a minimally invasive technique involving an endoscope. An endoscope is a medical device that transmits images via a long, thin tube and helps us examine the tumor.
After making a small incision in the nose or eyebrow, we will insert an endoscope, which has a very small camera on the end. Then we use microsurgical instruments beside the endoscope to cut out as much of the tumor as possible. We may restore the area with healthy tissue from elsewhere in your body, if needed.
Endoscopic Endonasal
Some tumors can be removed with the endoscopic endonasal approach. This allows our skull base surgeons to access tumors through the sinus and nasal cavities.
During either of your endoscopic procedures, we may need to temporarily install a spinal drain to divert any excess cerebrospinal fluid, prevent infection, and help the area heal. We will remove the drain a few days after your surgery.
Craniotomy
In a craniotomy, we will access the brain by temporarily taking out a piece of skull. We will draw back the exposed brain during surgery to reach the tumor. We use this approach when we can't reach the tumor through endoscopic surgery.
During a craniotomy, we may view the tumor with the help of a large surgical microscope. Scans from prior imaging tests, which we use as a guide, help us know the exact location of your tumor.
At the completion of surgery, the small piece of skull is usually replaced. Patients typically have a longer recovery time from craniotomy.
Lateral Skull Base Surgery
The standard treatment for lateral skull base tumors, such as acoustic tumors, is microsurgery. Common microsurgery approaches are:
- translabyrinthine,
- middle fossa, and
- retro sigmoid.
We make these approaches through an incision near the ear. We then remove the bone of the skull base to expose the tumor. Finally, we remove the tumor using the operating microscope.
In order to reconstruct the bone of the skull base, we may need to use an abdominal fat graft. This means we take a strip of fat from your abdomen.
Our team of doctors works together to remove the tumor and achieve the best outcome for you. Members of that team can include:
- a neurosurgeon,
- a neurotologist,
- an anesthesiologist.
Radiation
Stereotactic radiation allows us to sculpt the dose to the size and shape of the tumor without damaging nearby healthy brain tissue and the optic nerve. We may recommend radiation if:
- you aren't a good candidate for surgery because of your age and overall health.
- we need to target remaining cells that could cause the tumor to grow back.
- surgery is too risky.
We use a computer to calculate the appropriate radiation dose for your tumor. Your radiation treatment, which is delivered externally to your body, may require multiple outpatient visits.
- Stereotactic Radiosurgery -- This technique delivers radiation in one to five doses. No actual cutting takes place.
- Radiotherapy -- This technique delivers radiation in a larger number of doses.
Patients do not lose their hair and are often able to return to work the next day.
Chemotherapy
We rarely choose chemotherapy as a treatment for skull base tumors because most are benign. Chemotherapy is used to destroy cancer cells or prevent more from growing.
For some patients with acoustic tumors in both ears, we may recommend chemotherapy to keep the tumor from growing and keep your hearing intact.
Recovery After Skull Base Surgery
After surgery, patients may need to stay in the hospital for a period of four to seven days.
Medication can help relieve your pain and prevent brain swelling and seizure. Levels of exercise will vary, but many patients are encouraged to walk the day after surgery.
Our skull base surgeons will follow up with you to monitor changes in symptoms. More imaging tests will be needed.
Most patients are able to return to work and normal daily activities after recovery.
Contact the Destination Care Program
The Destination Care Program is an initiative by U of U Health focusing on care for our out-of-state patients. We are here to help you find the services and information you need. Feel free to contact us:
Email: DestinationCare@hsc.utah.edu
Phone: 801-587-6365